Course:
IMT Interview Questions Bank
You are the IMT1 on call. A 45-year-old woman presents to the Emergency Department with chest pain and shortness of breath.
Given the brief vignette, a wide range of differential diagnoses is possible. Therefore, a focussed history should aim to identify:
From the history, the patient reports sudden onset shortness of breath and pleuritic chest pain for the past 6 hours. She feels lightheaded and has noticed some swelling in her left calf over the last week. She has no significant medical history but she recently returned from a long-haul flight from Australia two days ago. She is not on any regular medications.
Primary diagnosis: Acute pulmonary embolism (PE) in view of the sudden pleuritic chest pain and shortness of breath in the context of leg swelling and recent travel. Other differential diagnoses to consider include:
I would initially assess the patient in an A-E manner. To refine my differential diagnosis, I would perform bedside investigations, including observations and ECG, and arrange blood tests and imaging, initially a chest X-ray and followed by a CT pulmonary angiogram (CTPA) scan.
Immediate actions:
Further actions:
Observations
| Heart rate | 124 bpm |
| Blood pressure | 1108/65 mmHg |
| Respiratory rate | 24/min |
| Oxygen saturations | 90% on room air |
| Temperature | 36.9°C |
Initial Investigations
| Investigation | Result | Normal Range |
| WCC | 8 ×10⁹/L | 4–11 ×10⁹/L |
| CRP | 2 mg/L | <5 mg/L |
| Sodium (Na⁺) | 142 mmol/L | 135–145 mmol/L |
| Potassium (K⁺) | 4.2 mmol/L | 3.5–5.0 mmol/L |
| Urea | 5.0 mmol/L | 2.5–7.8 mmol/L |
| Creatinine | 75 µmol/L | 60–110 µmol/L |
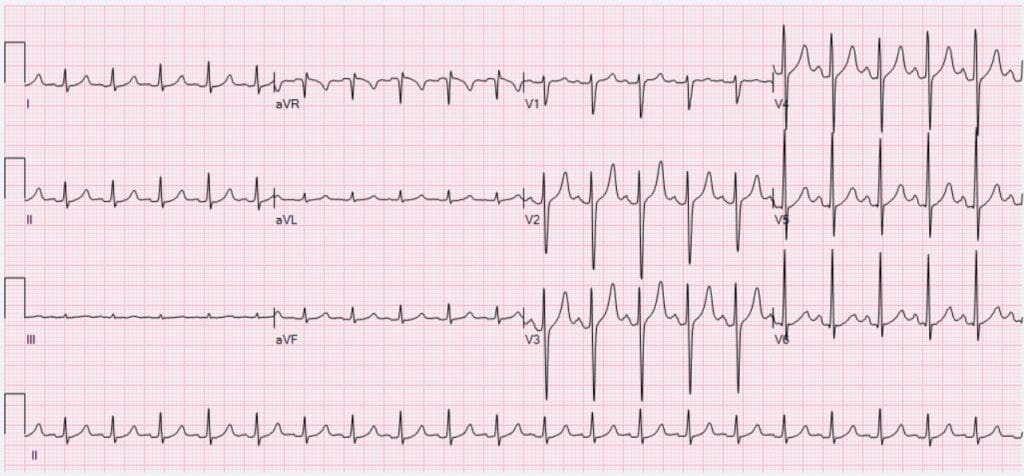
ECG
 Source: Ewingdo, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons
Source: Ewingdo, CC BY-SA 4.0 <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons
Chest X-ray
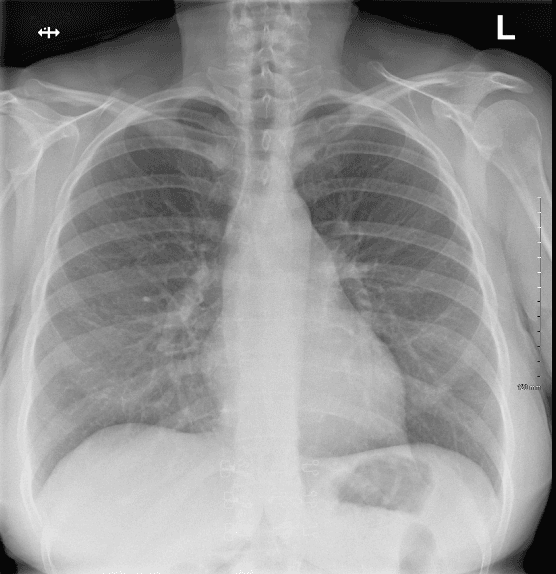
The patient is hypoxic, so would require hospital admission. Their current blood pressure indicates they are haemodynamically stable although they are mildly tachycardic. The blood tests presented are within normal range. No inflammatory changes are present and renal function is normal, permitting the use of oral anticoagulation. The ECG is consistent with sinus tachycardia with no ischaemic changes present. The chest X-ray shows clear lung fields with no abnormality present. These results have strengthened PE as the primary diagnosis. Therefore, I would proceed with arranging a CTPA or V/Q scan to confirm the diagnosis. In terms of the other differential diagnoses:
D-dimer tests are sensitive but not specific tests of thrombosis. Their value depends on the pre-test probability. In cases of low probability of PE, a negative result can be useful to rule out the disease. However, they are less helpful in cases where there is an intermediate or high suspicion of PE/DVT as it cannot safely rule out PE. In such cases, imaging to check for PE should still be performed.
Supportive measures:
Anticoagulation:
Thrombolysis:
Surgical or interventional options:
Patient and family
Colleagues
In the case of a suspected pulmonary embolism (PE), several scoring systems can guide clinical decision-making and risk stratification. The two-level Wells score can be used to estimate the probability of PE. A PE is unlikely in cases with a score of 4 or less.
| Clinical feature | Points |
|---|---|
| Clinical features of deep vein thrombosis (DVT; minimum of leg swelling and pain with palpation of the deep veins) | 3 |
| An alternative diagnosis is less likely than PE | 3 |
| Heart rate greater than 100 beats per minute | 1.5 |
| Immobilisation for more than 3 days or surgery in the previous 4 weeks | 1.5 |
| Previous DVT or PE | 1.5 |
| Haemoptysis | 1 |
| Cancer (receiving treatment, treated in the last 6 months or palliative) | 1 |
Another scoring system that may be useful is the HAS-BLED score to estimate bleeding risk on anticoagulation.
Situation
Hi, my name is X, I’m one of the IMT1 doctors. This is a 45-year-old woman presenting with acute onset shortness of breath and pleuritic chest pain. She recently returned from a long-haul flight and is hypoxic with oxygen saturations of 90% on room air.
Background
She has no significant past medical history but reports left leg swelling for one week. Initial investigations showed normal inflammatory markers and kidney function.
Assessment
She is highly likely to have a pulmonary embolism. We are arranging a CTPA but her haemodynamics are borderline with a blood pressure of 108/65 mmHg. She has received oxygen and treatment-dose LMWH. There is no evidence of contraindications to anticoagulation.
Recommendation
I recommend close monitoring of her haemodynamics. If there is deterioration, she may require thrombolysis or ICU-level care. Please arrange for an urgent review by the respiratory team if thrombolysis is indicated.